The same can be said about the actresses in the image below. Melissa Jaffer has a notably prolonged middle third of her face, and overall, her skull is convex (due to the maxillary rotational growth unopposed by resistance), compared to Abbey Lee, whose face isn't adenoid.
In comparison with the group above, these kids are not in caloric deficit, and thus they have a thicker layer of subcutaneous fat.
In your eyes, the second group of kids are completely normal-looking children. That’s what you see. I, on the other hand, see a doctor’s failure. Failure to educate the parents and, most importantly, the children about their adenoid faces and the imminent consequences of this condition. Doctor’s failure to act.
The boy in the pictures below is LANDON JONES. He suffers from a medical condition, which causes him to not feel hungry. Take a good look at the transition of his relatively good-looking facial shape to an adenoid face with severe convexity and downswing (more on the issue of crowded teeth later). Before the onset of this disorder, his diet wasn't perfect by any means - it consisted mainly of "fast foods" that weren't particularly tough. Still, his masticatory muscles were pretty well developed back then.
As the health condition set in, Landon stopped eating - he did not chew any food, so the maxilla rotated downward + backward (without any resistance in its way) and prolonged his face.
In the last picture, the boy appears to be sad/shy/grumpy - it's just an illusion (the rotated maxilla no longer supports the soft tissues of his face, and this leads to their sagging and his "sad" appearance). Take note of the hypotrophied masseters and a long midface after the unwanted transformation.
Read more here: (https://eu.desmoinesregister.com/story/news/local/kyle-munson/2014/10/26/landon-jones-medical-mystery-urge-eat-drink/17950935/).
Now, I will show you a perfect example of what happens when a person who didn't eat much food in his early childhood starts doing so in puberty.
This person is none other than DAVID LAID. For those who do not know, he is a fitness influencer known for his extreme body transformation, which positively changed not only his life but motivated millions of other people worldwide. What the majority of people do not realize is that it was not only his body that changed, but his face as well. Some will mistakenly argue that behind his altered facial appearance were pubertal hormonal changes (more on the effects of testosterone later...), but at this point, you already know better. It was the switch to a tough-food diet and ensuing frequent mastication that reorientated both of the jaws.
VARIANTS OF AN ADENOID FACE
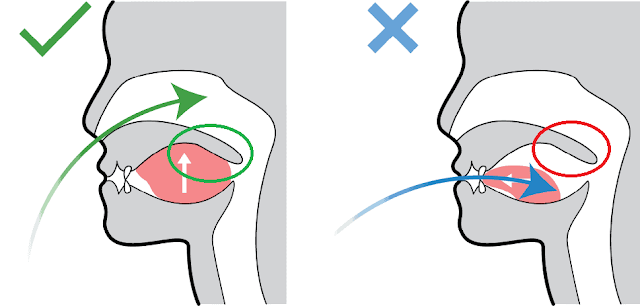
Do you remember when I said the tongue position still matters, even after we are born? Now it is time for you to find out a bit more about it. Among adenoid faces, we can recognize 2 main variants that depend solely on the tongue positioning.
Both of the men in the pictures below have adenoid faces, but there is a slight difference in their convexities. Liam Neeson has an adenoid face, but it is not as convex, compared to the person in the second picture. This occurs due to a phenomenon known as TONGUE-THRUST. It means, that the tongue is pushing from the inside of your mouth against your incisors, which makes them flare forward thus creating an illusion of buck teeth. Keep in mind that it is not only the teeth that end up flared forward but also a part of the jaw. Both upper and lower. This part is called the alveolar process, which you can see being pushed forward in the picture of me pulling my lower lip down. The majority of people, and sadly, doctors as well, assume that what they see is hypoplasia (underdevelopment) of the chin/mandible. Their failure in judgment leads to slip-ups in diagnostics and the following treatment. And who will be the victim in the end? You. The patient. The chin is never absolutely small; it can only be relatively small in comparison to the prominent alveolar process (it's anatomically impossible for the chin to be underdeveloped).
Tongue-thrust (Note that the tongue does not need to be positioned in between the teeth. In most cases, it only pushes on them):
Protruding alveolar process:
Both of these women have adenoid faces, even though the convexities are different. The face of the woman on the right is more convex due to tongue-thrust, and for the same reason, their chins seem to be of different sizes.
Their noses lack anatomical support from the rotated maxilla - that's why they appear to be large and curved (the nasal bone does support the soft nasal tissues, but the maxilla does not):
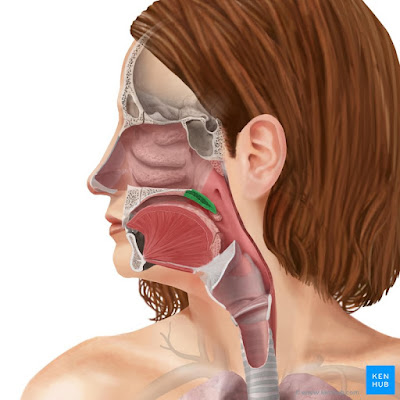
There is also a third variant of an adenoid face, but this one is extremely rare. Nonetheless, it should not be left out. This type is characterized by an ABSOLUTELY SMALL LOWER JAW (mandibular hypoplasia = underdevelopment, micrognathia). On the x-ray scans you can see why (+ notice the compensatory UPWARD HEAD-TILT):
The lower jaw of the patients above isn’t just pushed into downward and backward rotation by the growing maxilla, but it is extremely small at the same time. There can be multiple reasons behind it (all of them happening at a young age):
1) JAW JOINT ANKYLOSIS (Ankylosis means, that the temporomandibular joint becomes immobile, due to its ossification. Patient can barely open his mouth, let alone chew.)
2) CONDYLAR RESORPTION (due to trauma or arthritis, mainly idiopathic juvenile arthritis)
3) BURNS IN THE NECK AREA (Burns cause inflammation, which leads to the formation of fibrosis. Fibrosis then induces permanent contraction of the neck muscles. These pathologically altered muscles, along with the skin, pull the lower jaw downward, making chewing nearly impossible.)
4) NEVER EATING TOUGH FOOD - if one’s diet consists purely of soft food (minced meat, mashed potatoes, smoothies...), and he never chews anything in his life, the lower jaw will remain very small. Chewing stimulates the growth of our mandible. Notice the petite size of the mandibular ramus in the patients below (they didn't chew any tough food, and consequently, their ramus and the entire lower jaw did not grow = mandibular hypoplasia).
Their chins appear to be short, but that is only a result of the mandibular rotation and the tongue-thrust, which pushes the teeth and alveolar process forward. It is the entire mandible that is small, not the chin.
When we talk about rotational growth of the jaw, primary rotation occurs in the maxilla, and that in turn causes rotation in the mandible. Mandibular rotation is a little bit tricky, because there are 2 points of rotation.
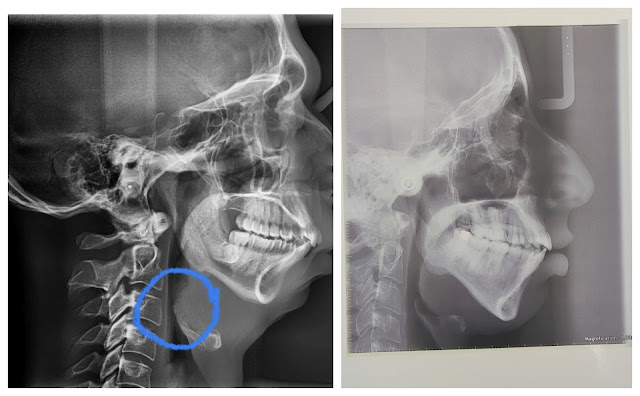
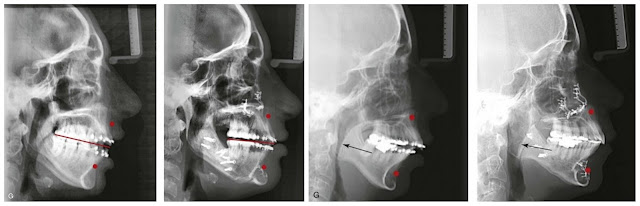
The first point is the temporomandibular joint itself and when rotation in this joint is anatomically no longer possible, the mandible will rotate in the second point. This one is located where the body of the mandible meets the mandibular ramus, as this place is the weakest point in our lower jaw. In most cases, you can find the second rotational point very easily, because it looks like a notch. This antegonial notch, along with the lengthening of apertura piriformis (see image below) and a prolonged midface, proves that the main cause of an adenoid face is in fact rotational growth of the maxilla and not only a lack of growth of the posterior part of the maxilla.
In the picture, you see an x-ray of my skull, and you can clearly identify the second point of rotation (you could also see it very well in some of the starving children):
My skull is the perfect tool for your learning. I want you to notice the slanted occlusal plane, optically enormous size of my nose, and protrusion of the alveolar process, which causes my lips to project forward and makes them more pronounced while making the chin look smaller. You see that
in my case, the mandible isn’t underdeveloped; it is just orientated differently. It's rotated. I do NOT have mandibular hypoplasia (micrognathia, small lower jaw), as I did eat tough food when I was a young child, but not frequently enough. Still, it stimulated the growth of my lower jaw, despite being insufficient to prevent the rotation in both of my jaws. Later, I will talk more in detail about the nose issue depicted here. See the difference in the soft tissues of my face after I rotated both of the jaws (so that the occlusal plane is horizontal) in the second image above.
One more time, to be sure you understand. The person in the first image below has an overdeveloped upper jaw (in a rotational manner) and an underdeveloped lower jaw (micrognathia) - he also compensates with an
upward head tilt for the lack of airway space. The person in the second image has an overdeveloped upper jaw (in a rotational manner), but the lower jaw is not underdeveloped; it's only orientated in a way that makes it seem smaller (explained on a piece of tube in the image below - the tube remains the same size; it has only been bent):
Compare the orientation of Hailey Kalil's
mandibular ramus and my mandibular ramus. In my case it is rotated posteriorly, while Hailey’s ramus points forward. This is a perfect depiction of the
first rotational point located in the jaw joint.
On top of that, the second point of rotation can be seen in my mandible as well.
TOOTH DECAY
Looking at the x-ray scan, you may also wonder why I have so many dental fillings. I digress here, but we will talk a little bit about tooth decay. The cause of dental caries is demineralization of the outer layer of our teeth (enamel). This enables bacterial infection to spread to the deeper layers of our teeth and thus leads to cavities and pain. The sugar in our diet serves as a source of food for the bacteria. The waste products of these bacteria are acids that break down the enamel. But that is not everything...
When I was a child, I always wondered why my teeth were so yellow, despite me religiously brushing them every day. My dentist told me it was genetics, which is, of course, a nonsense.
The teeth of every person should be of the color porcelain-white. If they are not, you can be sure the teeth are not mineralized, meaning the enamel is very thin, and through it, you can see the underlaying layer, the dentin. In adults, the yellow color may also be a result of external staining from coffee, wine, curry, and so on. For young children, external staining is out of the question, as their sustenance does not consist of these types of foods and beverages. So, when a child has teeth that are significantly yellow, it is always due to insufficient mineralization. In the image below, you can see me when I was little, and what seems to be an open-and-shut case now was sadly totally ignored by my doctors then.
Dentin has a naturally yellow color. In the picture, you can see what teeth with a lack of mineralization look like. Notice the
yellow color, glossy appearance, and
thin transparent line on the edges of the teeth.
Getting a lot of calcium in your diet is the key to addressing the issue here, but as always, it is never this easy. What every pediatrician should check up on are not only typical
clinical signs on the teeth of the child but also levels of
calcium and
vitamin D. Without this vitamin, the calcium that you ingest will never be absorbed in your guts and, therefore, will be lost.
We get the majority of vitamin D from exposing our skin to sun rays, so the majority of the population takes it for granted. Sunlight (UV-B) is responsible for the conversion of 7-dehydrocholesterol in our skin to vitamin D. In order to become active, it needs to be further metabolized in the liver and kidneys. Only then will you have an active form of vitamin D.
Rickets is the most severe form of vitamin D deficiency. Not every child will present with the typical symptoms if the deficiency is only mild. However, even in such cases, the teeth are still going to be negatively affected.
In addition, if maternal levels of vitamin D are below the normal reference range, it will also affect the tooth development of the fetus.
Similarly, vitamin K is also important in the context of teeth's health, as it helps with the accumulation of calcium in the teeth.

I am sure you have heard the saying "BLUE BLOOD". It‘s the blood of royals, and the reason behind it is that highborns did not spend much time in the sun compared to simple peasants working on fields; therefore, they had pale skin and the superficial blue veins were easily visible. You also heard that royal families used to have tooth decay more frequently than not-so-wealthy individuals. Yes, eating loads of sugar had a negative impact, but the primary cause was a lack of tooth mineralization due to vitamin D deficiency.
Sadly, dentists say that behind every cavity is poor oral hygiene, but the most important protection layer against bacteria is the enamel. Mechanical brushing will never remove all of the bacteria, and the ones that get left behind can still do significant damage. If the teeth aren’t mineralized properly in the first place, the demineralizing effect of the bacteria is amplified. In a scenario where your enamel layer is not mineralized and is thin, no matter how well you brush your teeth, you will still end up having tooth decay.
The general public believes that using tooth paste containing fluoride remineralizes the teeth. No, it doesn‘t. Calcium does that, not fluoride. Imagine your blood as an ocean, the calcium in it as a ship, and the fluoride applied on your teeth as a beacon. It helps to navigate the calcium deposition into your teeth, but when you are low on calcium, that is not going to happen. You have a beacon, but you don’t have ships.
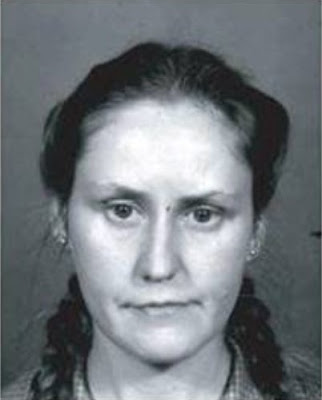
Take a good look at the yellow color of this kid’s teeth. Now compare them to his mother‘s porcelain-white teeth. The kid is starving and low on calcium; therefore, the formation of enamel is disrupted, and the yellow color you see is the dentin layer underneath it.
https://www.sciencedirect.com/science/article/abs/pii/S1879981717300499?via%3Dihub
Back to the main topic:
The critical detail that most doctors omit is that there is no clear line between the good-looking face and the adenoid face. Instead, there are as many DEGREES OF ROTATION as can be, hence numerous DEGREES OF DOWNSWING in our faces (do not confuse the degree of the downswing with the previously mentioned variants of adenoid faces). The extent of the downswing is a result of how frequently we masticate. And there is a difference between, let’s say, having tough food for breakfast + lunch + dinner and having tough food only for breakfast + lunch, but the dinner consists of soft food only. These subtle details, that do not seem like anything important, are in fact crucial.
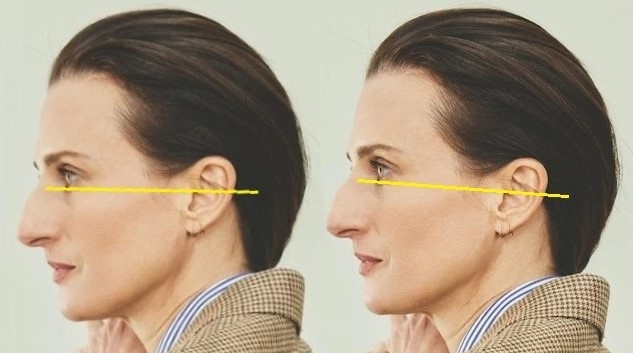
It seems that the woman below is fat; therefore, she has a "turkey neck". Wrong! She has an adenoid face and is subconsciously tilting her head upward as a compensation for compressed airways. Compenatory postural changes will be elucidated down the line...
Another important thing to note is AT WHAT AGE the child is introduced to the tough-food diet. Let’s compare the following 2 faces:
One of the guys is previously mentioned DAVID LAID and the other is JEFF SEID, also a fitness star. You already know that David only started eating tough food in his teenage years, and despite his face being very good-looking now, it is still visibly longer than Jeff’s face. In the picture, David’s mouth is slightly open, but it does not affect the outcome of their comparison. Jeff’s skull tells us he was introduced to tough food very early on in his life - the transition from being breastfed to eating tough food was seamless.
Notice that the second rotational point (notch) that is still visible in David’s mandible is not present in Jeff’s lower jaw. It's a tiny detail many would miss, but nevertheless, relevant.
Another seamless transition from being breastfed to eating tough food can be seen in Olivia Dunne. Having a tough food diet for her entire life after being weaned off breastfeeding allowed her to retain a very good-looking facial shape. Her
midface remained proportionally the same as she grew older.
The huge mistake that pediatricians, orthodontists, dentists, and people in general make when judging adenoid faces lies in the front teeth (incisors) of the child. Upcoming images serve as the perfect example:
Notice the kid in the right picture. I am sure you recognize him from a certain YouTube video in which he says that his peers laugh at his appearance and call him bunny. So his doctors decide to file down his incisors and give him braces (https://www.youtube.com/watch?v=thshr_PTgeI).
The issue is that his front teeth are not large at all. Behind this illusion of massive incisors is the slant in the occlusal plane, the tongue-thrust, and bad habits such as a tendency to put the tongue between the upper and lower incisors, lip-catch, thumb-sucking, or prolonged use of a pacifier.
Instead of filing down the kid’s teeth, doctors should have set him on a tough-food diet and given him braces only after the end of puberty to perfect the alignment of his teeth. What I am saying may sound like "pseudoscience" to you, but that was truly the only way to restore this boy’s face and his teeth back to normal. Chewing would not only stimulate the growth of his lower jaw but also gradually reorientate his slanted occlusal plane horizontally with the upswing of both jaws. The orthodontic work needed after that would be minimal.
NOSE
Many say that the way our noses look depends solely on our genetics. They couldn‘t be more wrong...
In the majority of people who have a recessed face, you will find that their nose seems to be a little bit out of place, with its large size and shape of a curved beak. It is only an ILLUSION. We do not inherit the shape of our noses. That is completely dependent on how much support the hard tissues of the maxilla and nasal bone provide to the soft tissues of the nose, including cartilage. At the base of the opening to the nasal cavity, is located one small bony projection called ANTERIOR NASAL SPINE (ANS). I added an x-ray scan of a person who has a good-looking face. Notice the ANS. It is in a relatively horizontal position, just like the occlusal plane, right?
Now take a look at the anterior nasal spine in my scans (marked red for better visualization). It is not horizontal at all; instead, it is slanted, just like my occlusal plane. Do not confuse ANS with cartilage (ANS is sharp and pointy, not dull)!
The anterior nasal spine serves as a support for the cartilage of the nasal septum, and so it is responsible for the shape of our noses. When the upper jaw is recessed, the ANS, as a part of the maxilla, is recessed as well. People with adenoid faces often have an aquiline nose (shaped like the beak of an eagle). That is no coincidence, but rather the sagging of the nasal soft tissues due to not having anatomical support. Sayings such as French nose, Roman nose, or Jewish nose are in fact based on a mere illusion where the person’s nose is not massive/hooked but rather his/her jaws are down-swung (hence the upper jaw doesn't support the soft nasal tissues - only the nasal bone does).
In the pictures, you see people who have large noses, at least at first sight. But look closely, and you will see that they simply have an adenoid face. The compensatory position of their head, which is tilted upward, creates the illusion of a prominent nose. I will explain the types of compensation later on...
In this trio of pictures, you can see how a wrong diagnosis always turns into the wrong treatment. The girl below had surgery performed on her nose and chin, but the end result isn’t satisfying anyway. Why is that? Because the real cause was not addressed at all. Instead of a nose job combined with the insertion of a chin implant, she needed a jaw surgery with counter-clockwise rotation of both jaws (at the end, I will provide more detailed information on jaw surgery). If you cover the bottom half of the third image, you wouldn't even say the girl has an adenoid face if you did not know beforehand.
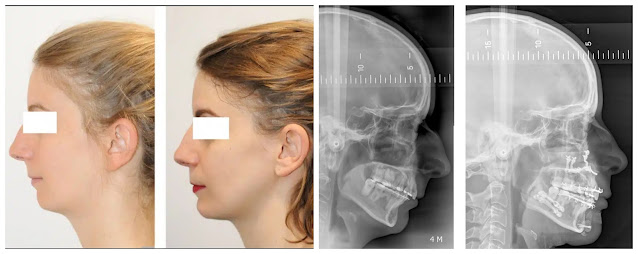
The image below shows the appearance of a person before and after the jaw surgery – this type of jaw issue is called CLASS 3 MALOCCLUSION (in the „genetics“ section, I will say more). Remember, NOT A SINGLE JAW ISSUE IS HEREDITARY.
Even though class 3 is not an adenoid face, you can see how much difference it made after the surgeon moved the maxilla forward, providing support for the nasal tissues. There was nothing done to the nose directly.
In the pictures below, you can see examples of pointless rhinoplasties (after the procedure, their faces are still convex, proving it is the maxilla that needs addressing, not the nose):
SKIN
Look at the following number of skin issues these people are bothered with, thinking the causative factors are age, genes, stress, and so on. But the real cause is simply a lack of soft tissue support by the maxilla and, subsequently, by the mandible.
The teenager below is also concerned with his appearance. Even though he is slim, his cheeks appear to be bloated. But his face is not bloated at all. It's just the skin hanging over the position where the maxilla (and mandible) should have been. Being lean and slim are two different things. He is skinny because he does not eat frequently enough, and his maxilla is rotated for the same exact reason. Significant reduction or even complete absence of mastication.
He says he has been chewing mastic gum for a couple of weeks now. Tough chewing gums are life-savers because, even when your financial situation does not allow you to eat tough foods every day, there is still a high chance you can afford this type of chewing gum. For example, from the brands STRONGER GUM, JAWLINER, or you can opt for mastic gum. Beware of using incisor-based jaw trainers, such as JAWZRSIZE, as these may cause an injury to the temporomandibular joint and lead to TMD. And so may chewing anything too vigorously... Muscles adapt to a heavy load fairly quickly, but if the jaw joint isn't used to frequent chewing, a sudden onset of rapid chewing will be stressful to the structures of the joint, which may lead to permanent damage. Patience and prudence are above everything here - it is imperative to CHEW SLOWLY (yet intensely)! Furthermore, it is not recommended using molar-based jaw trainers, for example, from the brand CHISELL. The main problem with these rubber gadgets (apart from the possibility that they may induce TMD like the previous type) is that while chewing on them, the occlusal contact is not being made. This will still allow the masticatory muscles to adapt through hypertrophy, but it will not lead to an upswing of the jaws. Physiologically, during mastication, the upper and lower teeth never directly touch, yet the jaws come fully together after each opening. This REPETITIVE OCCLUSAL CONTACT is necessary for the reversal of the down-swung jaws!
Remember, it is not about superficial reasons such as chasing sharp jawlines and looking like a "gigachad". Intense chewing in childhood and early adolescence will prevent and reverse the formation of an adenoid face - that is the goal you should aim for. In the linked article (
https://www.delish.com/food-news/a61158175/facial-gum-for-chiseled-jawline-teen-boys-tiktok/), Dr. Frank says that hard chewing gums are only a marketing trick and that defined faces come naturally as people age. That is not true.
Faces either develop correctly or don't, and the proper development of facial bones is guided by the masticatory muscles (and, in the earliest stages of our lives, by the tongue).
The boy is already 16, so he only has a couple of years at maximum for a positive change in his face. In order to achieve that, he needs to chew intensely every day in order to properly utilize this limited amount of time.

BODY DYSMORPHIA
In recent years, many kids have hopped onto the "mewing train". Their actions stem from an endless stream of TikTok, Instagram and YouTube shorts about defined jawlines and so-called "looksmaxxing". Sadly, most of these videos are nothing but a farce, spreading misleading, irrational content made solely for the purpose of receiving views and online fame. Undoubtedly, kids want to look good, but it's not only about appearance... Adults (teachers, parents) try to discourage their behaviour, linking it to the creation of a negative self-image, and instead encourage children to embrace their own "unique" looks, even when the issue is very clearly visible and should be addressed. Again, AESTHETICS EQUAL FUNCTION (HEALTH)! These kids see that something isn't quite right, so they try to change it for the better, but ignorant adults want to talk them out of it? Not surprising...
Equivalent to this situation would be a patient who's having typical symptoms of a heart attack. He walks into a hospital, and rather than helping him, medical personnel says: "It's only in your head. Don't you worry, everything is going to be all right." And in a couple of hours, he ends up dead...
Do you understand where I am headed with this? Kids are trying to improve their appearance and, with it, their health without even realizing it, and instead of providing them with useful information and our support, we suppress their efforts. Mewing (the tongue positioned on the roof of the mouth) isn't going to change anything - children need to be taught about the importance and necessity of MASTICATION.
Once I was waiting at a bus stop and a group of pre-school kids went by, all of them having recessed, adenoid faces. Usually there are only a couple of kids in every class, but this time it was the entire group. All of them. Situations like this bring tears to my eyes, knowing that it is medical professionals who are not doing anything regarding this serious health condition that dwells in our modern lives. Nowadays, we have doctors so that our children don't have to suffer from pathological health conditions like they did hundreds of years ago. What's the point of having your child assigned to a pediatrician who does not feel the need to prevent the formation of an adenoid face and, ultimately, its repercussions? It's like the kid visits the doctor only for him to treat infections, and the correct development of the child into a healthy adult is dependent solely on luck.
SNORING and OBSTRUCTIVE SLEEP APNEA


























































.jpeg)

.jpeg)
.jpeg)






























































































































































Very informative article.
ReplyDeleteIf I put my teenage son (15) through a rigorous hard food diet, would it be too late to see any changes, even if minimal?
At 15 years of age, the changes are still possible without a shadow of a doubt. If he stays consistent, he will be able to reverse the adenoid face.
DeleteI am also 15 year old guy have a long and narrow face caused by mouth breathing all the time then i consulted ENT and was diagnosed with adenoids so I'm doing treatment now and actively mewing. Can i reverse the face shape please reply 🙏
DeleteHey, this article is actually insane and mind-blowing. At first I was pretty skeptical, but you completely won me over cause it all made so much sense.
ReplyDeleteI'm turning 20 in 4 months and I wanna ask you if you've made any improvements with chewing in early adolescence, and how many hours a day you recommend chewing.
Again, good job on making this really good article and thank you for sharing it with us.
Thanks for the praise! As an adult (20 years old), you can expect only minimal changes, if any. Early adolescence is a different story, and that's not your case. No one will last a week looking at the clock while chewing; lifestyle alterations are necessary if one wishes to prevent/reverse the downswung jaws naturally (pretty much a complete change in diet). And sadly, it applies only to children and adolescents. Not adults.
DeleteYou claim that adult facial bones are unmalleable and unchangeable via muscle activity. How do you explain the fact that when an adult patient experiences a stroke and becomes paralyzed, we observe significant changes in facial skeletal form over time—most notably on the side of the face that is paralyzed?
ReplyDeleteWe observe changes in the soft tissues due to facial nerve damage (n.VII). Please be so kind and post a link to an image/video of the skull's changes in a patient after a stroke.
DeleteHi, first of all I just want to thank you. You are truly doing incredible work and it's really a shame that modern day medical professionals are so oblivious to this issue.
ReplyDeleteOne of my siblings is 15 years old and has an adenoid face. It's not likely that he can make a significant lifestyle change when it comes to eating harder food since our parents make all the meals we eat. Would it be possible to combat this issue with just mastic gum?
Hi, thank you. In such cases, tough chewing gums are the best alternative. Mastic gum is an excellent option, and on its own, it is more than enough. The scale of his results will depend solely on the consistency (intensity, frequency) of his approach.
DeleteIts remarkable how much time and effort has been put into this article. However, im still a bit sceptical. If u search on google "mason mount side profile" you can see that his mandible is downturned but he doesn't have that typical adenoid face look. His forward growth looks decent even though his jaw angle is very downward. You can't say that he looks like he has a recession. Why do you think that is?
ReplyDeleteHmm, so what you are saying is, braces or Invisalign can allign jaws and lips even after puberty? How is that possible if jaw development is over by that age? And even if they do work, wont they just push the maxilla in, making it look even worse and more recessed? How come Michael B Jordan and Mason Mount look much better after orthodontic treatment? How does one figure out if they should go for braces or orthognatic surgery.. since the latter isn't possible to the best extent after braces.
DeleteBraces/Invisalign align the teeth (that can be done at any age), but they do not improve the jaw situation. Moving teeth through the bone remodels it, but not favorably. If a kid or an adult ends up with a horizontal occlusal plane (achieved by braces) but the jaws are still recessed, it's essentially game over. The jaws cannot be up-swung anymore, neither naturally nor with jaw surgery. Michael B. Jordan and Mason Mount look better because, in people with adenoid faces, braces do 2 things: 1) They shorten the prolonged midface (which is a big factor when judging someone's attractiveness, but braces do not achieve an upswing of the jaws; it's only the occlusion that is moved upward, not the entire jaw structure). 2) Braces widen the dental arches, which makes the smile wider, hence more attractive (and the face looks more pleasing as well because the soft tissues are better supported by the widened dental arches). The answer to your last question depends on many factors and cannot be answered easily. One's individual needs and issues have to be considered, and giving you a universal answer is unreasonable.
DeleteI am a P.T and this was a very thorough text. I have also studied this topic and often encourage hard chewing to my clients. Its heartbreaking to see young children with recessed jaws because of the neglect of the parents. An interesting thing I noticed which was not mentioned in this article was that most children who have an "adenoid face" also have slanted/recessed foreheads. Would love to hear about your insights on this. Do you think rotation and upswing of the jaws will also change the shape of the forehead or is some other factor at play? I have seen cases of children reversing their downswing, fixing their posture and having a straighter forehead.
ReplyDeleteI would also like to add that tough chewing is important not only in childhood but also throughout puberty and even in early twenties.. I have seen cases where children were good looking till 16-17 or even 18 but then became "unattractive" due to bad habits and soft junk foods. As mentioned in this article, maxillary growth is very rare and difficult after 20, so its important to make tough chewing a lifestyle. Let me know if u agree!
DeleteThanks for reading my article. 1) I don't think it's a neglect of parents, but rather a lack of information (that should be provided by medical professionals); 2) slanted foreheads are only another illusion - take a look at the girl in the article who allegedly has "low-set ears". It seems that her forehead is also slanted, but that is only because she tilts her head upward. There is nothing wrong with the foreheads of these kids. 3) I do mention that mastication is important throughout childhood and also during puberty. Just look at the boy who was gifted a gerbil and then was marked as a "mouth-breather". In reality, he just stopped chewing for the entire duration of puberty. So chewing often as a child and then stopping at the beginning of adolescence is just as detrimental as not chewing in early childhood.
DeleteRealistically, till what age do u think people can expect noticeable results if they change their habits and diet? At what age would u suggest to not try and look into surgery, implants or other options. Great post btw, loads of value here.
ReplyDeleteThanks for reading it! As I mentioned in the article, one can expect changes until the end of puberty (approximately 20 years of age). The sooner the afflicted person starts, the better. Understand that not only age is relevant but also the approach of the said individual (intensity, frequency, consistency). Because of that, there is no definitive answer that would apply to everybody.
DeleteI really appreciate all the information you provided in this article, I'm sure it will help a lot of teenagers/adolescents like it did for me. I wanted to share my short journey and the results on a hard food diet. I'm 14 right now and although I'm not unhappy at all with my jaw shape/jaw line whatever, I wanted to read this blog to learn some more, and it was worth it. Only after reading into this that I realized I could feel the second rotation point in my jawline, and it was rotated downwards a little bit. I realized it was only a matter of time before it became noticeable. I read this blog about three weeks ago, and I've applied its ideas to my life and noticed small but still noticeable changes. I got these changes through eating a ton of fruits and vegetables like cucumbers and stuff every morning, as well as tougher meats etc. My question for the author is what foods should I mainly focus on specifically? I only got to eat a lot of these foods because I'm currently on vacation and the hotels have a buffet haha. Thanks for this article it definitely will change my life. Sorry for rambling and typing so much but I hope you will give it a read, and for other people questioning it, give it a try before you doubt it.
ReplyDeleteThanks for the encouraging words! I do not plan on giving examples of any tough foods, as these can be found easily through any search engine. However, the preparation of food matters more than the food itself - there is a difference between eating a steak and ground beef, yet fundamentally, it is the same food. Only preparation differs. I highly recommend investing in tough chewing gums, as these will save you money and not lead to an unwanted caloric surplus.
DeleteHello, have you noticed changes since its been a year?
DeleteHey! Funny I see your comment the one day I check the post. I'm 15, and yes I have made progress. Before my jaw was shortened to the point where I couldn't see the 2nd rotational point, but now I can pretty clearly see the 2nd rotational point since my jaw lengthened. My tip for you is: be careful chewing. I almost cracked my tooth cuz I was chewing mastic gum that was almost like chewing a rock. Chew hard gum but not too hard, and make sure you chew intensely, but also slowly, ensuring contact between your teeth (occlusal contact) so you can actually change your jaw through the force. I didn't see too much progress in my first six months of chewing because of two main mistakes: not making occlusal contact cuz the gum was too hard for me to bite through, and not chewing enough. There was a month period where I chewed between every single meal and that was when the most progress was made. Hope this helps :), so you can make the most of the time you have left and avoid the same mistakes I made
DeleteAnother thing I noticed is I can actually see my mandibular ramus now, before I couldn't even see it because my jaw was not short if u straighten it out but just rotated downwards so its shorter like that one diagram in the article if u know what im talking about. i dont know who you are but i hope this gives you hope, but keep in mind dont chew like a monkey, when i started i ignored Karols advice to chew slowly but intensely, and instead tried clamping my jaws together fast, which made my jaw a little funky. Luckily I stopped before it got serious. Goodluck on your journey bro, keep in mind it takes time, its not instant, and it took me well over a year since 14 to get here, and at 16 (I saw ur other comment) it will be even slower, but its a process. And dont lose hope, because you can still make a lifechanging transformation if you dedicate yourself at the age of 16. Be grateful you realized it now instead of when youre 18 or 20 when its too late.
DeleteHey man, I genuinely appreciate ur reply so much. I’ll take and try to apply ur advice to my journey, making sure I make occlusal contact between teeth when chewing hard gum and chew slowly plus intensely and don’t go crazy on it. By intensely I assume you mean pressure? And I’ll chew in between my meals. And what hard gum do you recommend? I’ve heard of falim mastic gum before, would that be great? Thanks for replying to me bro and I have this new hope within me that It’s possible for me to make a change.
Delete:)
Also, regarding diet, what type of food did/do you eat? Tough foods for example. I’m trying to incorporate a lot more tougher foods since I grew up on predominately soft food.
DeleteAdditionally , is there anything else you did to reverse the down rotation the jaw, or was it mostly/only tough chewing.
Appreciate it man.
I think I’m gonna get gum from the brand STRONGER GUM, that’s listed in the article. There’s 2 types of gum on there though there’s a hard gum (regular) or extra tough, which states: “• Hardest/toughest chewing gum in the world.
Delete• Stays tough when chewing, never becomes soft.
• Introduces your jaw bone and muscle to new types of grinding forces which causes bone and muscle growth.
• Contains a higher dose of vitamin D3 & K2 which is absorbed through facial tissue, assisting with the bone and muscle growth process.” But my mother doesn’t like the price. But just a quick follow up.
Hey, didn't see your thing sorry. Glad I inspired you with some hope, and yes intensely I mean apply pressure but don't shut your jaws really quick but not too slow either. For food, I eat hella steaks but it's not really something I worried about, since I focus more of my growth with chewing gum. I recently got STRONGER GUM, however I haven't tried it yet. I'm currently using JAWLINER medium toughness (the one that says 2x harder than regular gum) as I find it easy to make occlusal contact yet I can make it intense throughout. Beware of the ultra tough one, it felt like chewing a rock but idk, just my experience.
DeleteSo basically I recommend JAWLINERS medium toughness chewing gum which is packed in a normal chewing gum pack not the zip lock bag typa things, since it's the one I've made most progress with. I tried a few others, but this was my personal choice. I think STRONGER GUM is a solid choice too, but I'ma have to try it first.
For diet, I've been going to the gym before I read this article, and I started eating tougher foods and purposefully chewing tough foods, but I wouldn't worry bout it if you have the gum.
I did not do any other thing such as mewing or whatever. Only tried it during sleep like Karol recommended but I don't think about it tbh.
For the STRONGERGUM vitamin D3 and K2, the doses are kinda small tbh, idk if they'll do much but it's a nice bonus. I personally take vitamin d3 and k2 separately in pill form, 5000 IU (125 mcg) and 90 mcg of k2.
You said your mom doesn't like the price, which is completely fair. You can try explaining to her the importance, but mine didn't understand so I won't blame you. I made the money myself online and in-person so I recommend you find a way because your future self depends on it.
Hope this helps and answers all your questions :D
Quick follow up, I’ve just managed to order the medium hard gum you recommended from JAWLINER brand. Thought I’d let you know, and thank you for helping me with some advice and help man :)
DeleteHey, so it’s been abt a month I’d say since I’ve started, but I’m already on my last pack. I brought the 4 month supply pack (I’m pretty sure). Is this normal or am I definitely doing too much? How many pieces of gum did you use and how many throughout a typical day? I’ve been chewing in between meals so mostly 2-3x a day which 1-2 prices of gum, am I supposed to use only one? Sorry.
DeleteWAIT GUYS im a 14 yr old girl and idk if im done with puberty yet, im scared these stuff wont apply to me!! However im wondering is there a way i can stop the front of my jaw from moving downwards and potentially shorten my midface?. I have a gummy smile and lip incompetence so i thought i would get TADS to push gum up and fix my overbite potentially curing my lip incompetence & making my chin less recessed. Do you think that’ll work? And is there a way to pull the jaw upwards reducing the length of my midface naturally? 🥹
DeleteOmg i also forgot to say, i got diagnosed with an adenoid face!!
DeleteHey [red tangerine] so I’m sorry I can’t answer your questions as I’m not knowledgeable on that but no you are only 14 that is young and puberty is not over so definitely don’t worry about that. I think you should try what the article says if you think it applies to you
DeleteHey, It’s been a couple months now since August, and changes I'm not quite sure if there are any, but I do know that it will take a while of course, just wondering to myself when I will notice visible changes. Although I think I’ve developed tmj disorder or something along those lines. My jaw slips back and forth out of place every time I open my mouth, I’ve noticed. I don’t know if that’s a bad-bad thing or what.
DeleteAnd not to be weird or anything but [ mog man ] is there any social I can have just so I can keep in contact if I have a question if once in a while?
Idk how I’ve messed up but I swear I got TMD now - my jaw won’t open properly and I can see it come out the socket when I open it iykwim
DeleteHey, really nice article with precious info here. I have a question though, I had braces and now I’m wearing clear retainers nightly. Would my retainers and past braces treatment affect my gains from chewing?
ReplyDeleteIf you are not an adult yet and your occlusal plane is still slanted (braces did not make it horizontal), changes are still feasible. Wearing a retainer shouldn't hinder the upswing achievable via chewing.
DeleteHey, I found this article from a post on .org and I must say I didn't expect this much in depth information. The stuff here is deffo not half assed and the effort and time you put into this is commendable. I hope this post helps a lot of young guys and girls.
ReplyDeleteI am still confused between the relationship of downswung jaws and recession. If you take a look at Syrianpsycho (K Shami), you will notice that his mandible is grown downward and he has a relatively longer face, however there doesn't seem to be any issue with his forward projection. Do some people naturally have a larger gonial angles? Or am I mistaken somehow?
Thank you! Great question - I was hoping someone would ask this. In this context, recession equals downswing. The same thing that happened to "Syrianpsycho" happened to David Laid, whom I have covered in the article. Both of them started chewing later on after already developing a down-sung face. Hence, after introducing tough foods to their diets, the maxilla didn't shorten as much as it would otherwise be if the adenoid face never developed in the first place. That is why I compared David Laid to Jeff Seid, and you can see that Jeff's gonial angle is more acute compared to David's. But, you also see that Olivia Dunne never developed down-swung jaws, and yet her gonial angle isn't as acute as Jeff's gonial angle (Jeff's ramus is longer). So why is that? It's because Jeff used to chew a lot more intensely (and frequently) when he was younger, unlike Olivia, who chewed just enough to prevent the downswing (intense mastication stimulates the growth of the ramus). Take a look at this linked image (https://imgur.com/gallery/skull-male-female-chewing-intensity-hAIy6e9). The skull above represents what happened to Jeff, and the skull below represents what happened to Olivia. These differences in the mandible have nothing to do with gender/sex hormones, but only with the intensity of chewing. I hope this covers your question.
DeleteThis comment has been removed by the author.
DeleteOne of the most important blog ever. I really wish this information was more mainstream and orthodontists actually gave this advice.
ReplyDeleteYou mentioned that poor posture is caused by an adenoid face and never the reverse. Does this mean that it isn't possible to correct posture using stretching exercises (like psoas stretches) and breathing exercises to fix rib flare which is often the underlying cause for forward head posture and APT.
I appreciate it! The exercises you mentioned are necessary in order to correct the posture, but if the cause (down-swung jaws) isn't addressed, the bad posture will most likely relapse, as the airways are going to remain compressed. What I meant is that having bad posture will not cause/worsen the downswing of the jaws.
DeleteYeah, thats understandable but what about someone like me who is in his adulthood with an adenoid face. Is working on my posture pointless since itl relapse anyway? I dont think I want to get an invasive and painful jaw surgery since I never had any noticeable breathing problems.
DeleteIt definitely isn't pointless, but keep in mind that your body will always try to find a way to compensate if the downswing in your case is severe. By performing certain stretches, you are alleviating the symptoms, but their true cause is left untreated.
DeleteHello. just read the article. I've had Braces when i was 11 and took it off while 12, which left me with few years of retainers that i put on while asleep. Thing with my braces was that even though i had overbite, i didn't did any work on bite issues or 'fine tuning', i just did Stage one of braces about 12 months. Now, im 13 years old, will chewing hard foods frequently help even though i had braces? is there any other alternatives or anything? I got downswung jaw.
ReplyDeleteHi. For the chewing to facilitate the upswing of the jaws, the occlusal plane has to be slanted. If braces have made your occlusal plane horizontal, chewing will not help you. Your age is not an issue, as you are still very young.
DeleteIn general, do braces always positively change the appearance of a face? If not, what kind of adenoid face is worsened by braces and which kind is bettered. (Only talking from an aesthetic point of view as I have a downswung face similar to mason mount or Bellingham but no breathing or postural problems and deep bite teeth.)
ReplyDeleteBraces do not benefit anyone with an adenoid face (down-swung jaws). It may seem like they do, as the maxilla is shortened vertically, and then the teeth + the maxilla provide better support for the lips and the rest of the soft facial tissues, but the mandible isn't brought up (it remains down-swung), along with the maxilla and the occlusal plane. If you do have an adenoid face, you most definitely have breathing issues (people with down-swung jaws don't even realize they have problems because they compensate for the worsened airflow with the 3 compensatory types I mentioned in the article - most compensate by tilting their head upward, and this isn't something you are aware of as it is subconscious).
DeleteGood day to you man. This is an amazing piece of work!!!
ReplyDeleteI am only 15, and while I don't have an adenoid face, I do have a malocclusion (specifically - deep bite.)
I have heard a lot of people talk about Invisalign and how it doesn't cause as much pain as braces. Infact, my dentist told me that Invisalign will be sufficient for my teeth. Even so, im confused whether to go for it or stick to braces.
Is there any downside to Invisalign ? Will it be just as effective as braces in fixing my teeth as well as shortening my maxilla and improving my lip allignment and soft tissues as u mentioned above for braces.
Also you mentioned that upswing of jaws is not possible after the occlusional plane is made horizontal by braces. Is the same true for downswing? If I get braces right now, I probably wont be able to chew as many hard foods. Could this cause a downswing of jaws or will the horizontal occlusional plane mean no more movement will occur?
DeleteHi. I am not going to give you advice on how to address your deepbite, as my article focuses only on the topic of an adenoid face (and deepbite is a separate jaw issue). What I meant was that chewing ensures that the upswing of the occlusal plane is simultaneous with the upswing of the jaws. You are young, hence your jaw bones still continue to grow - if you won't chew, there will be no resistance against the natural rotational growth of the maxilla, and that will lead to a downswing of both jaws. Braces/Invisalign alter the positioning of the teeth, not the jaws. And these appliances will not prevent the natural downswing of the jaws; only chewing will.
Deletethis is an amazingly articulated blog and really great to read, thank you for taking the time to write everything.
ReplyDeleteim not sure if this is really related to the post but how does ramus length tie into this, i notice that my ramus isnt as long as i would of liked it to be, and so far ive attributed that to genes, however my jaw is down swung and i don't believe i have an adenoid face (but i am biased i know). do you think ramus length has anything to do with this maxilla rotation?
Hi. A similar question was asked by a commenter "jackiesst" above. Chewing stimulates the growth of the ramus, making it longer and more robust. Here's a link to an image that compares 2 skulls (https://imgur.com/gallery/impact-of-mastication-on-length-of-mandibular-ramus-DcYxR1i). The jaws are not down-swung in either of these skulls, and yet you can see the difference in the length of the mandibular ramuses. The reason why the skull in the x-ray scan has a shorter ramus is that the patient used to chew enough to prevent the downswing, but not as intensely and frequently as the hunter-gatherer in the second image. And no, genes do not affect the jaws at all.
DeleteThis was a very interesting read for sure. I like how everything was explained one by one almost like a book! I had a couple of questions.
ReplyDeleteFirstly, are there any long term complications that come with having a subconscious upward head tilt? I've noticed a lot of people nowadays have it. Especially younger people.
Secondly, the part about tooth decay was very eye opening. As an older kid or adult what can someone do to restore healthy teeth? I don't just mean whitening since there are a lot of procedures for that.. what I mean is, can someone older thicken their enamel layer?
Chronic upward head tilt will reflect in bad posture overall, which may lead to other complications down the line.
DeleteNo, once the teeth erupt, the process of enamel formation is complete, and after that point, the enamel cannot be regrown or regenerated.
Could you explain a bit more about tongue thrust and how it affects the face? Judging by the article it seems like tongue thrust actually saved those people from developing an even worse looking face due to slight maxillary and mandibular projection. Are there any negatives to a protuded alveolar process?
ReplyDeleteAlso can someone with a short mandible also benefit from chewing to lengthen it or will chewing only facilitate upswing? (im 17 hoping to see changes in my face. I have strated regularly chewing stronger gum.)
DeleteOnce I posed this exact question to a more erudite person than myself, and the answer was that the teeth may eventually fall out due to a lack of support. However, I am not sure how much credibility this answer holds.
DeleteMandibles are short only relatively (I explained it on the piece of tube in the article). The upswing will lead to more forward projection; hence, the mandible will appear longer, but in reality it's just going to be oriented more horizontally.
Definitely a great read! I have a few questions I'd like to pose.
ReplyDeleteCould hard chewing potentially damage the teeth? I read somewhere that vigorous chewing of mastic gum can damage molars and you might need to get molar implants. I also asked my orthodontist about hard chewing and explained to him the science behind this. He was very dismissive and he claimed that it will give me tmd.
I also wanted to gain a final clarity on braces and Invisalign. Do they or do they not affect the positioning of jaws in an adenoid face. Iv come across several sources which state that braces actually push in the maxilla creating a sunken look. Why then do people like Bellingham and Michael B Jordan as mentioned above by others not face these consequences? Is it simply a myth that braces push the jaws inwards?
Lastly I'd like to ask you about orbital recession. What do you think causes it? Is it simply a side effect of having an adenoid face or is it genetic?
I assume by damage you mean the teeth getting worn out. This wear can be seen in the skulls of all hunters-gatherers; however, with our modern diets, it's never going to happen. Teeth grinding (bruxism) is a different story - due to a lack of airway space, patients grind at sleep, and during nighttime, the "buckshot reflex" (during mastication, if the upper and lower teeth come in contact with something way too hard, the whole process of chewing suddenly stops) isn't present. This way the patients are damaging not only their teeth but also the temporo-mandibular joint (masticatory muscles contract and push the condyle head deep into the socket, which results in loss of circulation for some time). Progressively, the jaw joint will get damaged, and the result is TMD. Fast / vigorous chewing may also cause TMD; hence, chewing at a slower pace is recommended. But chewing gum isn't going to cause any damage to the surface of the molars.
DeleteRegarding the treatment with braces, it really depends on the specifics of the treatment (e.g., usage of TADs or previous tooth extractions), so I cannot give you a clear answer as each treatment is individual and there is no way for me to know the details of every case. Braces mostly push the jaws inward in people who have had extractions.
Orbital recession is caused by the downswing of the maxilla along with zygomatic bones, which are in direct contact with it.
As regards this informative study, you have mentioned any children, especially adolescents, should incorporate mastication practices with intensity, consistency and frequency, providing that they are urge to reverse those down swung face. While the post recommends tough gum as an optimized alternative, many mainstreamed papers and channels really propose against the long-term use of them, (cavity, tooth decay, bloating, GERD, ...) and only suggest a short 15-minute daily chewing instead.
ReplyDeleteTo what extent do you think this is a piece of misleading information or rather a verified scientific proof? Is it advisable for adults (20s)?
Thanks for the post!
Thanks for the question. It all comes down to the ingredients used in the gum. The companies selling tough chewing gums are aware that chewing regular gum frequently can lead to tooth decay; hence, they opted for xylitol as a main sweetener. Xylitol, unlike sugar, doesn't lead to cavities; moreover, it has protective properties.
DeleteSo appreciate you for this 🙏🏿🙏🏿🙏🏿. Have you come across the effects of tongue tie in your work?
ReplyDeleteIf primary mouth breathing is caused by inflammation in the airway, does that mean the true root cause isn't lack of tough food but the source of the inflammation (ex. Gerbil)?
How did you handle your food intolerance to eat more?
The root cause of adenoid faces is natural rotational growth of the upper jaw. If one doesn't chew, there is no resistance opposing this growth, and the formation of an adnoid face takes place. Inflamed airways are never the cause. The tongue tie should obviously be resolved, but in toddlers and older children (whose source of nutrition is solid food instead of liquid), it plays no role in the development of down-swung jaws.
DeleteTongue tie would restrict the infant from properly swallowing amniotic fluid, thus causing the downward rotational growth of the jaw, correct?
DeleteHello, I just want to start off and say this was a great read so good job on that!! You already said this in your article briefly but there’s really is absolutely nothing you can do once your occlusal plane is horizontal ?? I’m sorry but my jaw is downswung and I already went thru the whole braces treatment for quite some time unfortunately and I think my occlusal plane is straight but I always thought that maybe some kind of surgery with CCW rotation can save me but reading this is making me think otherwise 😭 I don’t mean to make you repeat yourself but not even surgery can fix you after that and can you explain why ? 😞 Once again sorry and thank you for the article 🙏
DeleteAs an OMF surgeon, I can save OP some time and repetition, (can delete this if you want) -
DeleteBraces make the occlusal plane horizontal. In bimax + ccw, we rotate the jaws along with the occlusion to achieve an upswing. This is simply not possible if orthodontic work has already made the occlusion horizontal. The jaws cannot be rotated independently. As mentioned in the article, this is sadly a major flaw in today's orthodontics.
However, not all hope is lost for you :) Braces don't always make the occlusion completely horizontal. If it is slightly downswung, ccw rotation of the mandible and maxilla is still possible to some extent. Your best bet is to get evaluated by a surgeon. Even in the unfortunate case that your occlusion is indeed horizontal, a simple bimax with advancement may help alleviate sleep apnea or other issues you may be having (although this isn't guaranteed and depends on your individual case.) From an aesthetic standpoint, custom implants, genioplasty, targeted fillers, rhinoplasty, orbital implants etc. can help you obtain a more balanced profile even if your jaws are downswung.
Best Regards - Lahm Kaiser
Hi Karol first of all what a thorough and conclusive article. I am 36 with adenoid face and had kids 4 years ago so have been in the process of getting my life together to be my best for them. Ive quit drinking and smoking 3 years ago, and I exercise every day. Your article explains me perfectly. The face, crooked teeth, obstructive sleep apnea, forward head posture and anterior pelvic tilt. Ive been separately searching for answers not knowing these are all connected. CPAP machine for sleep, invisalign with 4 teeth removed after losing 2 teeth 10 years ago, and lower back ache due to APT so o know focus some exercise toward this. Is there anything i can do??? Please help, your article is so good and yet made me sad to read and confirm i am an exact subject of your writing
ReplyDeleteThanks! As for the APT, focus on consistently stretching the psoas and simultaneously strengthening the muscles that are relatively weak (core muscles, glutes, hamstrings). And instead of relying on CPAP, look into jaw surgery for the OSA. I cannot give you a more comprehensive answer as I haven't seen you in person.
DeleteI found this article randomly on .org and i must say that this is very impressive and down to every last detail . i have a couple of questions tho . so basically im 15 and 6 months old right now and i got braces from 13 and removed them just 6 months ago , but i was very ill disciplined and i did not properly put on my elastics ( thats if i ever put them at all since i found them annoying ) , and i stopped wearing my invasilign after 2 months even tho the doctor told me to put them on for 2 years , i think the doctor put some type of wire on my lower and upper incisors to prevent them from getting back to their original position . i wanna say that i grew up hating red meat and most of my diet consisted of soft foods and chips which caused me to get an overbite and i was bullied for having rabbit teeth . after braces id say that my jaw became more developed and my teeth became aligned BUT my chin is unfortunately recessed and i developed very bad posture with forward neck tilt and an anterior pelvic tilt ( this bad posture mainly occured cuz of my prolonged gaming sessions which i also had bad posture in ) . im just asking to see if there is any ray of light for me to fix my recessed chin and bad posture since you said that chewing will have zero effect if you had braces . thanks for such an amazing article and it really made me more self aware than i already was and i will definitely try my best to provide my children with a hard food diet and help them develop better habits . i also wanna say that im sorry for my terrible wording since i skimmed through your article and only understood the basics of it .
ReplyDeleteChewing may still benefit you if your occlusal plane (OP) remains slanted after the treatment with braces. Braces do not make the OP horizontal in everyone with down-swung jaws. As for your chin, it's not recessed/small. The issue lies in the rotation of both the jaws, and perhaps your alveolar process is projected forward too much. There is no way for me to know more without pictures or x-ray scans, so this response will have to suffice.
DeleteHello. Your blog was an interesting read. I have a 9 year old daughter. She has lip incompetence, and an overbite. Her mouth is very crowded, and after reading your blog post it seems she has a very small mandible. She was a very low birth weight baby, did not take to solid food for a long time, and struggled with constipation that probably restricted her food intake, she was in miralax for a very long time.
ReplyDeleteShe has recently had her adenoids removed, and she is being seen by a Myofunctional speech therapist. She has also been seen by a two orthodontists, both whose opinion was that she is still skeletally immature, and will take a wait and see approach until she’s older. One said he would put in a spacer for about a year, but not yet.
It occurs to me after reading this that correcting the overbite is a band aid fix for the underdeveloped mandible. Now I will not leave my daughter with these issues untreated as she wants them fixed, but I am certainly curious in what else I can do.
It seems from your blog the solution is a tough food diet. I really don’t think her current diet is terrible by any means, they eat fresh fruits, veggies, meats, breads, ect. What can I do to help her? Increase tough foods even more? What are your thoughts on gum, or that hard chewing gum? How long and often would that need to be chewed for?
Lastly if I were to implement any of these changes, how long do you think it would take to notice positive changes so I can evaluate if it’s working or not?
Thank you.
Hello, and thank you for reaching out. Myofunctional therapy is a great first step to take. As for the tough chewing gum, I think that tough foods are sufficient for her age. A lot of parents think that their child is a "big eater", while it doesn't have to be the truth at all (during my pediatric internship I came across such situations, and the children in question were undernourished) - so incorporate more tough food into her current diet. If you choose to opt for a chewing gum, I recommend mastic gum due to her young age. The best advice I can give you without seeing your daughter in person (or at least her x-ray scans) is to get her to an orthodontist who works with Myobrace appliances (these will also help with the tooth crowding). Here's a link to a transformation of a child who underwent orthodontic treatment with Myobrace (https://imgur.com/gallery/myobrace-appliance-MkAPp9k).
DeleteWow thank you for this. You are doing great work for the youth. I have a Question, I had braces from 13 to 15 (now) can i still see change from chewing? I had no extractions. Also should I wear my retainer during the day/ night?, as that limits the teeth's ability to move and I want to make space for my wisdom teeth. Also how long should I chew mastic gum daily for to see changes and make room for wisdom teeth?
ReplyDeleteHello,
DeleteI can answer some of your questions as I have asked similar questions to Karol before.
1. Would I see changes from chewing?
Whether you will see a change depends on whether your orthodontic treatment had straightened your occlusal plane already. If your occlusal plane was originally slanted but it has been straightened through orthodontic treatment, I am afraid that changes cannot be made already.
2. How long should I chew everyday?
Unfortunately, Karol does not have an answer for that yet. However, I am in the same age group as you and these are what I have done:
I switched to a hard food diet with about 45 mins a day of chewing across 3 meals. I have started around the 8 months ago and now, approaching 16, I have seen that my face has became more squarish but changes to my crooked teeth and occlusal plane is still not yet visible.
3. Should I wear my retainer during the day/ night?
This is a tricky question as the wrong advice might cause more harm than good. If you value your orthodontic treatment and current state, you should keep doing what your orthodontist recommends. However should you gamble away the treatment you paid in hopes of getting straight teeth naturally again through Karol's findings, do note that this is quite unrealistic. You are already post 15 and like me, have only limited time left for changes. I am not in a position to dictate the best outcome for you.
This is my humble reply to your comment and please note that I am not in any situation to give medical advice to you. I am too, trying to make as much changes as possible. - Mr Wong
Thanks for replying, my main goal is to make room for my wisdom teeth, I am actually happy with my face and most definitely do not have an adenoid face, however I want to make room for my wisdom teeth because all the ignorant orthodontist here want to take everyone's out. What do you think I should do? Also did you see any changes in your zygomatic/cheekbone area? When switching to chewing alot.
DeleteThis comment has been removed by the author.
ReplyDeleteThank you so much for this article. After reading this I can finally open my eyes to my issues. I was always confused how I had a downswung maxilla/jaw since I don’t mouth breathe. My diet throughout my life has consisted of so much soft food, minced meat, yogurt, potatoes, etc. If I adapt to a tougher- chewier diet with steaks, carrots, apples and mastic gum etc. will I able to reverse the damage that’s already happened. I’m 16 with an adenoid face, is it over regarding my down swung jaw. As a younger kid I was handsome, with lots of potential for beauty, however as I’ve grown up with the terrible habits and no information regarding this I’ve developed poorly and look unattractive. Please.
ReplyDeleteHello Hostile dog, I am also 16 and in the same boat as you. With regards to if you will be able to reverse all the downswing completely, I am not certain but I am sure that if you maintain a consistent hard food diet, you will see changes, firstly with an increase in massater muscle size.
DeleteYou seemed very concerned over your looks, which I truly understand as someone who used to envy those with forward grown faces that they somehow had the causes for a hard food diet.
As I grew older I rationalised that this 'beauty' they have is just a manifestation of an optimal jaw position, something which everyone should have become. I stopped fantasizing about what 'it could have been' for me when I reduced the attachment of my self worth on my looks by understanding that everyone, even those with good looks will look grow old and frail eventually. It is just a matter of time. Being good looking is like a candle in the wind; it burns brightly but is fleeting. You might try various means to become 'good looking' e.g. chewing hard foods, jaw surgery... but if you do not address the underlying insecurity of not being able to be comfortable in your own skin, those external changes may not bring the fulfillment you seek.
Wow this post is amazing. I also have an adenoid face and was a very picky eater as a child. Now that I have my own kids, I want them to reach their full potential. My 4 year old has a beautiful jawline, but my 2 year old has a recessed chin already. Thanks to your blogpost, he still has a chance to a having nicely developed face. I appreciate your extensive research and providing your knowledge with the internet!
ReplyDeleteI am also 15 year old guy have a long and narrow face caused by mouth breathing all the time then i consulted ENT and was diagnosed with adenoids so I'm doing treatment now and actively mewing. Can i reverse the face shape please reply 🙏
ReplyDeletePlease read the parts on chewing again, mewing ain't going to fix anything
DeleteIf i’m 17 is is too late to fix this?
ReplyDeleteIs it too late to reverse minor rotation at 17?
ReplyDeleteYou would be able to achieve results before your growth ends. A good indicator of you going in the right direction is that your masseter muscles will hypertrophy.
DeleteBut will it do anything to my actual bone rotation, besides the soft tissue.
DeleteIf you haven't stopped growing, it is physiologically possible for actual bone rotation. Unfortunately I do not have the expertise to identify if your growth has stopped or not
DeleteI have a question on if how you chew matters. Would chewing with the pre molars/ incisors vs the molars make any difference. If you recruit more of the temporalis and deep masseter muscles rather than the superficial masseter will that have an affect? Do the two different muscles affect the bone structure in any different way? If your masseters are tight and you dont massage/stretch them could that lead to any negative effects on rotation/structure? People mention chewing upward and forward. Is this necessary and what does that mean? I understand not chewing side to side and upward but i dont understand how youre supposed to chew forward. Also should i focus on using lots of force while chewing and should my teeth touch during chewing? Any help would be greatly appreciated
DeleteI have a question on if how you chew matters. Would chewing with the pre molars/ incisors vs the molars make any difference. If you recruit more of the temporalis and deep masseter muscles rather than the superficial masseter will that have an affect? Do the two different muscles affect the bone structure in any different way? If your masseters are tight and you dont massage/stretch them could that lead to any negative effects on rotation/structure? People mention chewing upward and forward. Is this necessary and what does that mean? I understand not chewing side to side and upward but i dont understand how youre supposed to chew forward. Also should i focus on using lots of force while chewing and should my teeth touch during chewing? Any help would be greatly appreciated
ReplyDeleteHi Adam, thank you for this most enlightening article- you mentioned that TmD problems can arise due to downswung jaws. We have completed a MARPE treatment for my 17 year old daughter, but due to her TC syndrome and underdeveloped mandible, she slay has had condylar resorption during her early teen years. However, now we see that her condyles have stabilized. Her airway is narrow and she needs jaw advancement . We have some surgeons telling us she needs her entire hard joints replaced, and some surgeons telling us that just a BSSO is enough. And yet other surgeons that are proposing an inverted L Osteotomy. What are your thoughts in her case? I would love to speak to you directly as well. Thank you
ReplyDeleteThank you deeply for writing this. The appreciation I have for you taking the time to write this cannot be expressed in the pixels shaping these digital words. Probably the best thing I've ever read.
ReplyDeleteIf you do happen to ever come back to this and see this, I would love to know your thoughts on the Reviv mouthguard, the creator(ken)'s theories and claims, similar mouthguards, the balloon theory, and that nature of stuff. Thank you
ReplyDeleteHey, i read your article recently im 17m, in my country we eat rice mainly and soft food and its not possible for me to change it currently. We also dont have mastic gum to buy in the country. So without any alternatives i am thinking of getting molar jaw trainers, those silicone blocks to put in between your molars on both sides, will they be effective and safe? or just a waste of time and unsafe?
ReplyDeleteHello I understand your situation. As Karol stated, these molar jaw trainers do not allow contact between the teeth while chewing so it would not result in any upswing. The hard foods which I intentionally incorporate into my meals are uncut raw carrots, almond nuts or apples. If you eat soft rice frequently, you can add almond nuts in your rice and voila! Each bite becomes chewy.
DeleteI can see that the author hasn’t been active on here as of late, but I have a question if he or anyone has any advice..
ReplyDeleteI’ve been chewing for around 5-6 months now and I must have been chewing wrong (too fast most likely) and have developed a funky jaw, which I think is TMD.
My jaw cannot open properly and I can see it slide outta place as I open it. My parents advise me to discontinue the gum, however, I of course don’t want and will not be doing that as I want to try the hardest to reverse the downswung jaw. What should I do, and is continuing it with tmd safe?
Hello hostile dog, I think we have a lot in common concerning rotated jaws and in the same age range so we can dicuss more about our situations on google chat, or email me directly at wonghonwen@gmail.com
DeleteTo answer your point, you should give your jaw some rest if not you could mess it up lol.
Hey again, alright thank you.
DeleteThanks for the contact too.
Sorry for late response
I haven't read the whole thing but I'm working on similar issues. It would be great to get in touch. My site is jawhealth.org or you can see my case at breathingetc.org:3600.
ReplyDeleteHi, I think the author Karol Adamik has not returned to this site in a long time so it is unlikely that he would see your message soon. Please read this article fully though, it contains many ideas deviant from the mainstream jaw epidemic activists with his reasons.
DeleteHey. Please help, Karol, or anyone. I got braces almost a week ago. I HATE them. I feel as though it is making me uglier and is a gamble for my face. When I read what braces does, what would happen if I remove them now? Does it affect my gums? Guys, please please help.
ReplyDeleteAlso, is the change reversible? Let's say after a month or 3, if I remove them then, can my teeth go back into its original shape? If I remove them by myself now, does my teeth go back to normal, or am I getting myself into a bigger problem (ie my teeth becoming even worse?)
Lastly, what do y'all think about REVIV? It's a new concept and I'm considering buying it. There's huge success stories, but the lack of science behind it is making me very uncertain.
Hello Rose, it is normal to be concerned about how you look after you get your braces. However, the main purpose of Karol's blog is to address the issue of the misconceptions around adenoid faces, and not about orthodontics.
DeleteYou talked about how you hate braces and feel as though it is making you uglier + it is a gamble, and I understand why you would think that way. The thing is, Rose, it depends on the reason why you need braces. If your orthodontic treatment is done to camouflage a skeletal issue instead of being just dental-alveolar, you definitely would look better after treatment, but not addressing the root cause of the issue.
To answer the question if the change is reversible, I will say that yes, it is. Teeth are constantly shifting back to its original position if there is originally a skeletal deficiency which is not addressed.
You talked about how teeth get back to its original shape, and I don't really understand what you mean by that. What did they do to your teeth size? Did they shaved them down?
My two cents on reviv is that it is not a substitute of actual research on airway orthodontics or medicine. Time spent dealing with reviv is better off coming to peace with the fact that you are kind of stuck with the face you have unless you have deep enough pockets to seek the likes of treatment as seen in JawHacks.
By the way, I am 15 and female. I am scared my window for growth is disappearing.
ReplyDeleteTo put it plainly, yes, once your maxillae growth plates have ossified, there is nothing you can do non-invasively to alter the downward growth.
DeleteThey also shaved a tooth on my lower jaw and all my front teeth dont touch anymore, just the back teeth. I really really need help. I am desperate to take these off, I emailed my ortho but no response yet. I may just have to remove the brackets by myself to prevent further shifting. The pain from braces is gone now, but I'm afraid the roots of my teeth are already dissolving and moving.
ReplyDeleteI'm sorry that I wasn't able to reply you sooner. Perhaps, you could share more about your situation through email? You might not want to expose too much personal information which cannot be easily removed here. My contact is ai_yuqi@tutanota.com, feel free to drop me an email.
DeleteInteresting article, most of this I really agree with, however there is excellent evidence that oral posture, ie the position of your tongue, lips and jaw gap all have an impact. Also, the sutures between the bones never truly fuse and appositional changes in the bones is always possible. Well done and very informative. It amazes me how many people are now talking about this, one step at a time, we need answers and better solutions. Mike
ReplyDeleteHello Mike, it is quite evident that oral posture has an impact on facial development. However, rotated jaws is specifically caused by lack of maxillary resistance through chewing post infancy, and not oral posture with reasons as stated in the blog.
DeleteTo convince me with your theory about cranial dystrophy, could you:
1.Provide me evidence which isolates oral posture being able to cause maxillary downswing in humans without chewing?
2.Provide CBCT images which show that sutures never truly fuse?
Thank you for reading my message.
Yu Qi